Dementia
Dementia is a progressive neurological condition that affects memory, thinking, behaviour, and the ability to perform everyday tasks, profoundly shaping the lives of those diagnosed and their families.
As symptoms worsen over time, people may lose their independence, require increasing levels of support, and experience significant emotional and social challenges. The impact extends beyond the individual, placing substantial physical and psychological demands on carers and communities.
Dementia also carries a considerable financial cost: health and social care services, informal caregiving, and long‑term support collectively represent one of the most expensive areas of care within health systems.
Together, these personal and societal burdens highlight the importance of early support, coordinated care, and continued investment in prevention and research.
Range of visuals describing dementia and its impact (Source: Alzheimer’s Research UK)
Local approach for Dementia
Wirral
On Wirral, we are now progressing into the next phase of our work to complete the Dementia 100 Pathway Assessment Tool through a number of workshop sessions led by the Dementia Working Group.
These sessions are chaired by AGE UK Wirral and supported by the Cheshire and Merseyside Integrated Care Board.
This collaborative approach will be a collective effort to review and populate the assessment tool in a structured, collaborative way, with contributions from partners across Wirral essential to ensuring the information captured is accurate, comprehensive, and reflective of current practice across the Wirral system.
This page will host future improvement plans and developing evidence, so return back to see updates.
Cheshire and Merseyside
Cheshire and Merseyside Dementia Strategy: 2025 - 2030
NHS Cheshire and Merseyside, and partners, recognise that as a region where people living with dementia—and those who care for them—can live well, feel supported, and remain connected to their communities.
This sub-region strategy is not intended to be just a document; it is a call to action to ensure that every person affected by dementia receives the care, respect and opportunity they deserve.
Dementia Friendly Liverpool City Region Pledges
The Dementia Friendly City Region Pledge commits each Liverpool City Region (LCR) Local Authority to:
-
Commit to having lead Dementia Champions identified within their organisations.
-
Form and be enthusiastic members of Local Dementia Action Alliances (LDAA) to help transform the lives of people with dementia and those that care for them; and bring about a society-wide response to dementia through member action.
-
Work collaboratively with service user forums and advocacy groups to take action on issues identified as a priority by service user reference forums for dementia and engaging with service user advocacy groups as part of this process.
-
Engage with voluntary, community and faith organisations and the business community to mobilise the social capital within the local economy, to connect communities and ensure communities are working together towards the same aims.
-
Promote dementia awareness and understanding to address the stigma of dementia through LCR wide awareness campaigns and local community events and information sessions.
-
Provide Timely information and advice to ensure that people across LCR living with dementia and their carer’s are provided with appropriate information, at the right time, and have access to ongoing support to navigate the ‘dementia journey’.
-
Embed a collective commitment to train and develop a Skilled Workforce across LCR Councils and partner organisations to support people living with dementia and their carer’s. 8. Share best practice, knowledge and understanding of current themes affecting dementia services across LCR to Drive continuous improvement in local services and facilities. 9. Work with partners to ensure people living with dementia and their carers have Access to early assessment and diagnosis so that treatment and support can be initiated as soon as possible, to enable people living with dementia to maintain a good quality of life. 10. Listen; where individuals and their carers have told us that our systems don’t work, we will work with our partners to provide Local Integrated Services that offer seamless, wrap around support, built around people not organisations.
Next Steps
Wirral is continuing to strengthen its local approach to dementia by undertaking the Dementia 100 self assessment, a comprehensive review that helps organisations understand how well current services are meeting the needs of people living with dementia and their carers.
This assessment supports the identification of strengths, gaps, and opportunities for improvement, enabling more consistent, efficient, and evidence based dementia care across our local system. It also encourages collaboration by sharing good practice between services and informing future commissioning and service redesign.
Alongside this, Wirral Council is working with partners to develop and deliver a strategic plan for dementia that addresses the wider factors influencing dementia risk, progression, and inequalities.
This work aims to ensure that our services, places, and communities are dementia friendly and inclusive, with a focus on key themes such as awareness and education, co production and lived experience, access to services, the built environment, technology and innovation, carer support, health and prevention, and community engagement.
Updates will be shared on these areas of work as they move forward.
Dementia 100 Pathway Assessment
Dementia 100 is a national tool designed to help local areas in England understand how well they are supporting people living with dementia and their carers. It is used by NHS teams, councils, and partner organisations to check the quality of dementia services and identify where improvements are needed.
More about Dementia 100
Although the tool itself is for professionals, its purpose is entirely centred on improving the day-to-day experience of people living with dementia.
The format of the Dementia 100 tool is an evidence based self assessment framework made up of 100 criteria that describe what good dementia care should look like across the whole dementia journey—from prevention and diagnosis to end of life support.
It brings together national guidance, standards, and best practice into one place so local systems can assess themselves consistently.
What the Dementia 100 Tool aims to achieve
Improve the quality of dementia care
By reviewing services against its 100 criteria, local areas can see what is working well and what needs improvement—helping ensure people receive high quality, person centred support.
Reduce variation in care
Different parts of the country often provide different levels of support. Dementia 100 helps create more consistent and fair dementia services wherever someone lives.
Support better planning
The tool helps organisations plan future dementia services, making sure they match what people need locally. It guides strategy development and service redesign.
Encourage partnership working
The tool emphasises integrated, joined up care—encouraging NHS, social care, voluntary organisations, and community groups to work together.
Highlight good practice
Areas doing well can share their approaches with others, helping raise the standard of dementia care nationally.
Dementia 100 - Six Pillars for improvement planning
Understanding Dementia
Dementia is a degenerative brain disorder that disrupts memory, cognition, behaviour, and everyday functioning, significantly affecting the lives of those who develop it as well as the wellbeing of their families. This section looks in more depth at the condition and its impacts.
What is Dementia?
Dementia is an illness associated with the progressive decline of brain function. A key symptom of dementia is memory loss, and while consciousness is not affected, the impairment in cognitive function is commonly accompanied, and occasionally preceded, by changes in mood, emotional control, behaviour, or motivation.
Dementia can be caused by a number of diseases which destroy nerve cells and damage the brain, known as neurodegenerative diseases, which cause cognitive decline beyond the level expected with normal ageing.
Dementia has physical, psychological, social and economic impacts, not only for people living with dementia, but also for their carers, families and society at large. There is often a lack of awareness and understanding of dementia, resulting in stigmatization and barriers to diagnosis and care.
Dementia, while most common in older ages groups, can also affect younger people. Young onset dementia, sometimes referred to as early onset dementia, is generally defined as any type of dementia that develops before 65 years of age, often occurring in those aged 45-65.
World Health Organization (WHO) recognizes dementia as a public health priority.
In May 2017, the World Health Assembly endorsed the Global Action Plan on the public health response to dementia 2017-2025.
The Plan provided a comprehensive blueprint for action – for policy-makers, international, regional and national partners, and WHO in the following areas: addressing dementia as a public health priority; increasing awareness of dementia and creating a dementia-inclusive society; reducing the risk of dementia; diagnosis, treatment and care; information systems for dementia; support for dementia carers; and, research and innovation
International key facts
- In 2021, 57 million people had dementia worldwide, over 60% of whom live in low-and middle-income countries. Every year, there are nearly 10 million new cases.
- Dementia results from a variety of diseases and injuries that affect the brain. Alzheimer disease is the most common form of dementia and may contribute to 60–70% of cases.
- Dementia is currently the seventh leading cause of death and one of the major causes of disability and dependency among older people globally.
- In 2019, dementia cost economies globally US$ 1.3 trillion, approximately 50% of these costs are attributable to care provided by informal carers (e.g. family members and close friends), who provide on average 5 hours of care and supervision per day.
- Women are disproportionately affected by dementia, both directly and indirectly. Women experience higher disability-adjusted life years and mortality due to dementia, but also provide 70% of care hours for people living with dementia.
The scale of the challenge
In 2024, dementia was the leading cause of death in the UK[1].
There are an estimated 944,000 people in the UK with dementia, with an estimated 1 in 11 people over the age of 65 having the condition[2]. In 2024, England had a record high number of dementia cases, reaching 483,000 by December 2024[3].
Prevalence is driven primarily by population ageing. Risk rises steeply with age, and the number of people aged 85+ continues to grow rapidly across all regions of England.
The number of people diagnosed with dementia is set to rise, in the UK it is estimated that by 2051, there could be 2 million people living with dementia[4].
Dementia represents a major and growing challenge for Wirral, driven by an ageing population, persistent inequalities in health outcomes, and sustained pressure on health, social care and unpaid carers.
In 2026, dementia already shapes demand across primary care, hospitals, adult social care and the voluntary sector, and its impact will intensify over the next decade unless mitigated through prevention, timely diagnosis and effective support.
Demographic change alone means dementia prevalence in Wirral will continue to rise even if age‑specific risk remains stable. This will likely increase demand for memory assessment, post‑diagnostic support, home care, carer support and residential care.
Types of dementia
Age-related dementia
Dementia is usually categorised as ‘young onset dementia’ if the individual affected is under the age of 65 years old, with dementia occurring above this age deemed ‘late onset dementia’.
Young Onset Dementia
Early onset dementia, also referred to as ‘young onset’ dementia, refers to any type of dementia that occurs in an individual under the age of 65. There is no minimum age that somebody can start to exhibit symptoms of dementia with the condition developing at any age, although it is most often between 45 and 65. Young Dementia Network state that there are 60,000 people living in England with young onset dementia. There are estimated to be 92 people per 100,000 of the population diagnosed with dementia between age 30-64. People with a learning disability are at greater risk of young onset dementia. One in ten may develop Alzheimer’s disease between the age of 50 to 65. The number of people with Down’s syndrome who develop Alzheimer’s disease is greater with around 50% developing symptoms in their 50 to 60s.
Dementia over 65
Dementia that affects people older than 65 years of age can sometimes be known as ‘late onset’.
There are over 100 different types of dementia known to exist. Information on the most commonly recognised types of dementia can be found on the following pages – including Alzheimer’s Disease, Vascular Dementia, Dementia with Lewy bodies and Frontotemporal Dementia.
Mixed Dementia
Some people have more than one type of dementia. The most common combination is Alzheimer’s disease and vascular dementia, which is caused by problems with the blood supply to the brain. Another combination is Alzheimer’s and dementia with Lewy bodies (DLB). If a person has mixed dementia, they will show symptoms from each type of dementia that they have. This means a person with Alzheimer’s and DLB might have problems with their memory (Alzheimer’s disease) as well as problems with movement and alertness (DLB)
Most recognised types of dementia
Alzheimer’s Disease
Alzheimer’s disease is the most common and well-known disease that causes dementia, accounting for 60-70% of all dementia cases. It is characterised by a build-up of proteins in the brain which affect how the brain cells transmit messages. As time passes, more brain cells are damaged, leading to worsening symptoms. The most common early symptoms include memory problems, thinking and reasoning difficulties, language problems and changes in mood – although other symptoms can occur in the later stages.
Vascular Dementia
Vascular dementia, also known as “multi-infarct dementia” or “post-stroke dementia”, is the second most common cause of dementia. The symptoms include memory loss, impaired judgment, decreased ability to plan and loss of motivation. Vascular dementia is caused by damage to blood vessels in the brain.
Blood contains oxygen and nutrients that help brain cells to work properly. When blood vessels are damaged, less blood reaches the brain. This can affect how brain cells work. If this damage spreads, over time it can lead to symptoms of vascular dementia.
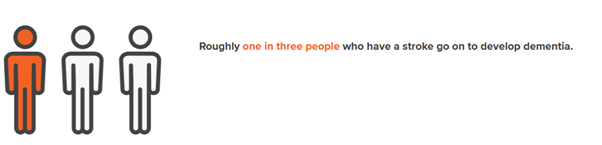
Strokes are a common cause of vascular dementia. Although a single stroke can cause vascular dementia, it is more likely to develop after more than one, or multiple, strokes – although people who have a stroke are more likely to have more strokes. So, they have a higher risk of developing dementia in the future.
Dementia with Lewy Bodies
Dementia with Lewy Bodies (DLB) is the third most common cause of dementia; also known as “cortical Lewy body disease” or “diffuse Lewy body disease. Symptoms can include sleep problems, memory loss, hallucinations and frequent swings in alertness. Lewy bodies are abnormal proteins that somehow appear in nerve cells in the brain, impairing its function. The exact causes as to why Lewy bodies appear are not yet fully understood.
DLB is closely linked with the development of Parkinson’s disease, with the build-up of Lewy bodies is also found in Parkinson’s - but in different areas of the brain.
Frontotemporal Dementia
Frontotemporal dementia is rare. This type of dementia is also known as “frontal lobe dementia” or “Pick’s disease”. Unlike the types of dementia noted above, frontotemporal dementia is marked more by behavioural and emotional changes than by cognitive impairment. In fact, memory is often preserved in people with frontotemporal dementia until much later stages.
Symptoms include decreased inhibition (frequently leading to inappropriate behaviour), apathy and loss of motivation, decreased empathy, repetition of compulsive behaviours, as well as anxiety and depression. Frontotemporal dementia occurs when the frontal or temporal lobes of the brain are damaged or shrink.
LATE Dementia
Not to be confused with ‘late-onset’ dementia, LATE (or limbic-predominant age-related TDP-43 encephalopathy) dementia is a comparatively recently discovered type of dementia, recognised as a clinical entity in 2019.It primarily affects older adults, particularly those over 80, and is characterised by memory and cognitive impairments. The characteristics of LATE are very similar to that of Alzheimer’s disease making it very difficult to diagnose. This discovery also helps to explain why the development of a cure has been so problematic for scientists.
Posterior Cortical Atrophy
Posterior cortical atrophy (PCA) is an uncommon type of dementia that usually begins by affecting a person’s vision. It is also known as Benson’s syndrome, ‘visual variant’ or ‘visual-spatial’ Alzheimer’s disease. PCA is caused by damage that builds up in the brain cells at the back of the brain. This is the part of our brain that processes information from our eyes, and allows us to make sense of what we are seeing and where things are.
Primary Progressive Aphasia
Primary Progressive Aphsaia (PPA) is a rare type of dementia cause by damage to parts of the brain that control language, personality, emotions and behaviour. PPA affects the left frontal lobes of the brain more, this is where our speech and language are processed. In most cases, PPA is caused by frontotemporal dementia.
It is important to note that just about any condition that causes brain or nerve cell damage can also cause dementia. For example, people with Parkinson’s disease will often exhibit dementia in the later stages of their illness. Huntington’s disease, Creutzfeldt-Jacob disease and alcoholism may all lead to cognitive impairment.
Why invest in dementia?
Dementia imposes a huge emotional and financial cost. As the number of people with dementia rises so too will the costs for the health and care system, as well as the individual’s families.
A series of reports commissioned by Alzheimer’s Society in May 2024 showcases insights into the economic impact of dementia.
Key findings include;
-
The cost of dementia in the UK is forecast to be £42 billion in 2024, rising to £90 billion by 2040.
-
The average per person costs associated with mild, moderate and severe dementia are estimated to be £28,700, £42900, and £80,500 respectively, with increase in cost by severity driven by increasing need of complex care.
-
The growth in dementia means that, by 2040, there will 6.9 million additional primary care contacts associated with dementia, requiring an estimated 1.7 million more hours of primary care time.
-
People with undiagnosed dementia attend A&E on average 1.5 times per year, which is higher than attendances for diagnosed mild, moderate, and severe dementia patients, and three times higher than attendances for patients without dementia.
-
There are interventions that can keep people well for longer and in their own homes.
-
For AChE inhibitors: Though these treatments are not effective for everyone, for those in whom they are effective at slowing cognitive decline there is a potential saving of up to £8,000 - £45,000 per person through delayed admission to care homes.
-
Unpaid care is the largest driver of cost, followed by social care.
Although, local authorities and NHS organisations are under increasing financial pressure, investment in dementia care is vital to ensure appropriate, effective management of the condition (before reaching a crisis point) and to provide support to families and carers in order to maintain their own health and wellbeing.
For local health systems, introducing improved dementia prevention and interventions will:
-
contribute to cost savings across the health and social care system
-
support people to live longer and healthier lives
-
reduce the risk of developing a number of other long-term physical conditions, such as hypertension and heart disease as well as mental health conditions such as depression
-
impact on costs associated with non-communicable diseases such as heart disease or stroke
-
transform the future of society
What does the data tell us?
Dementia is an illness associated with the progressive decline of brain function. A key symptom of dementia is memory loss, however dementia also effects mood, movement, judgement, language and more . Dementia can be caused by a number of diseases which destroy nerve cells and damage the brain, known as neurodegenerative diseases, which cause cognitive decline beyond the level expected with normal ageing.
Facts, figures and trends
Technical Report (April 2026)
Dementia Workshop PowerPoint Slides (November 2025)
What are the views of local people, communities and stakeholders?
Qualitative insight from people with lived experience of dementia is essential, offering depth and context that data alone cannot. Hearing directly from individuals and carers helps reveal real‑world challenges and priorities, ensuring services are shaped around what truly matters to those affected.
As new insights are gathered they will be added to this section.
Local
The development of the Dementia 100 work will lead to a wider engagement and involvement with local residents including those living with dementia, both those diagnosed and families providing support.
This page will be updated as and when new insight is available.
National
The lived experiences of dementia (2025)
‘Left in the dark’ - One in five people affected by dementia get no support: the true impact of dementia laid bare | Alzheimer's Society
This lived experience survey captures the voices of almost 3,500 people affected by dementia, including those living with the condition, unpaid carers and loved ones. It finds that one in five people affected by dementia have received no health care, social care or financial support.
Of those who received support, fewer than half were satisfied with it, with only 29% saying dementia-related health care was easy to access. More than half believe this situation could be improved if increased support from professional carers trained in dementia was available.
International
International Evidence on the Impacts of Dementia: Perspectives of People Diagnosed and Their Families
This document summarises international evidence on the impacts of dementia from the lived experiences of people diagnosed with dementia and their families. The content is suitable for use in Joint Strategic Needs Assessments (JSNA), policy development, and strategic planning.
Impacts on People Living with Dementia (Lived Experience)
Emotional and Psychological Impacts
- International qualitative research consistently shows that receiving a dementia diagnosis is experienced as both a relief and a shock.
- For many individuals, diagnosis provides an explanation for cognitive and functional changes and reduces confusion, shame, and self-blame.
- At the same time, it introduces fear, uncertainty, and grief about the future. People commonly describe anxiety about loss of independence, distress linked to changes in identity, and concern about becoming a burden on others.
Social and Functional Impacts
- Across countries and cultures, people living with dementia report progressive restrictions on social participation and everyday activities.
- Individuals often experience reduced confidence in managing daily tasks, withdraw from social roles, and become increasingly dependent on family support as symptoms progress.
- Global evidence highlights that people with dementia value opportunities for adaptation, rehabilitation, and continued participation in community life, yet access to such supportive and person-centred services remains limited in many health systems worldwide.
Impacts on Families and Informal Carers
Emotional and Relational Impacts
- From an international perspective, dementia is widely described as a relational condition that affects the entire family.
- Family members, particularly spouses and partners, experience a profound sense of loss as they witness gradual changes in personality, communication, and shared relationships.
- This process is often described as a ‘loss of the person before death’. Emotional impacts on family carers include chronic stress, grief, guilt, sadness, and feelings of social isolation.
Role Changes and Caring Burden
- Families frequently take on complex and demanding roles, becoming primary caregivers, care coordinators, and advocates within fragmented health and social care systems.
- International qualitative studies highlight that carers often feel unprepared for these responsibilities and report limited access to clear information, coordinated services, and ongoing professional support.
- The cumulative burden of caring can negatively affect carers’ physical health, mental wellbeing, employment, and financial security.
Impacts on Children and Younger Family Members
- International research demonstrates that children and young people affected by parental dementia face distinct and often overlooked challenges.
- These include emotional distress during prolonged periods of uncertainty before diagnosis, premature caring responsibilities, and disruptions to education, social life, and future aspirations.
- Evidence suggests that young family members often feel invisible within adult-focused services, highlighting the importance of whole-family approaches to dementia support.
Inequalities and the Global Context
Low- and Middle-Income Countries
- Globally, people living in low- and middle-income countries face particular disadvantages in relation to dementia.
- These include delayed or missed diagnosis, limited access to post-diagnostic support, and heavy reliance on unpaid family care.
- Such gaps place significant emotional, physical, and financial strain on families and often amplify gender and socioeconomic inequalities, as caring responsibilities disproportionately fall to women.
Stigma and Cultural Factors
- Across regions, stigma remains a major influence on the lived experience of dementia.
- People living with dementia and their families report discrimination, social exclusion, and being excluded from decisions about care and daily life.
- In many cultural contexts, fear of stigma leads families to conceal diagnoses and delays help-seeking, further increasing isolation and unmet need.
Key Cross-Cutting Themes from the International Evidence
International evidence consistently highlights several cross-cutting themes.
- Dementia affects identity, relationships, and wellbeing, not only cognitive functioning.
- Families experience cumulative and long-term emotional and practical impacts.
- Early diagnosis alone is insufficient without sustained post-diagnostic, relational, and psychosocial support.
- Person- and family-centred approaches, grounded in lived experience, are critical across all stages of dementia and across diverse health and care systems.
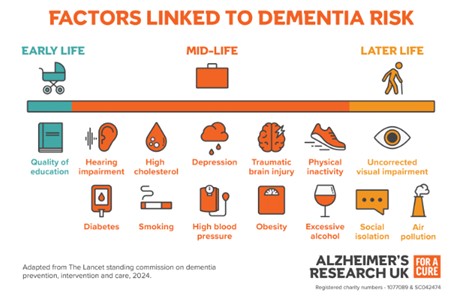
Who is risk of dementia and why?
There a range of risks including older age, certain genetic factors, and health or lifestyle issues, such as cardiovascular disease, smoking, or inactivity, and these can all increase the risk of dementia. As risk rises, the effects extend beyond the individual, often placing significant emotional and practical pressure on families who provide support and care.
Who is at risk?
Older People
The World Health Organisation (WHO) that the strongest known risk factor for dementia is age: the older you get the more likely you are to develop dementia.
Dementia is not an inevitable part of ageing, however, we do know that the risk of developing dementia increases with age - and dementia can also be young onset (symptoms developed before 65 years of age). Alzheimer’s Society explains that ageing as a risk factor for dementia may be due to factors associated with ageing, such as:
• Changes to nerve cells, DNA and cell structure
• Weakening of the body’s natural repair systems
• Higher blood pressure
• Changes to the immune system
• Loss of sex hormones after mid-life changes
• Increased risk of cardiovascular disease
Younger People
Alzheimer’s Society suggests that there are over 70,800 people in the UK are living with young-onset dementia. Someone who is diagnosed as a younger person might be concerned about the effects this will have on their family, relationships, finances and daily life. They may also be worried that any children or siblings will have a higher risk of developing dementia.
Gender
Dementia statistics by Alzheimer’s Research UK reveals that only 35% of people living with dementia are men compared to 65% women. One of the reasons for this is likely to be due to women’s longer life expectancy. While some studies have suggested that other factors may affect the number of men and women with dementia, there is no firm evidence that women are more likely than men to develop dementia at any given age. Women are more likely to be dementia carers than men and this often leaves them feeling isolated and depressed – a risk factor in itself for dementia.
Ethnicity
More recent research has found that people from ethnic minority groups face a higher risk of developing dementia. A study by Queen Mary University in 2022 found around 1 in 10 cases of dementia were linked to ethnicity, and a similar number to socioeconomic deprivation (population attributable risks of 9.7% and 11.7% respectively) – even after adjusting for modifiable risk factors like smoking, weight and vascular health.
Stressful and traumatic life events have been linked to dementia, so it’s thought that issues like racism and poverty-induced stress could play a role in raising the risk of the disease among these groups. These numbers could also be partly because of the vascular risk factors found in Afro-Caribbean and South Asian UK populations for illnesses such as hypertension, high blood pressure, diabetes, stroke and heart disease. It is also important to note that ethnic communities are under-represented in dementia services and are therefore less likely to be diagnosed or are diagnosed at a later stage. Reasons for this could be due to communication issues, cultural bias and lack of awareness about the condition.
Down’s Syndrome and Learning Disabilities
The prevalence of dementia is four times greater among people with a learning disability according to the UK Health Security Agency.
Down's syndrome, also known as Down syndrome, is a genetic condition caused by an extra copy of chromosome 21 in cells. This typically causes some level of learning disability and characteristic physical features. Research has also acknowledged that the additional copy of this chromosome contains a gene that produces proteins involved in changes in the brain caused by Alzheimer’s, which is why it is believed that those with Down’s syndrome have a higher risk of developing dementia.
It is currently estimated that there are around 21,199 adults in England and 115 adults in Wirral with Down’s Syndrome (POPPI and PANSI, 2019). The Alzheimer’s Society estimate that 1 in 50 people (or 2%) with Down’s Syndrome develop dementia in their 30s. This rate rises to more than 50% for people with Down’s Syndrome who live into their 60s, compared to the estimate of 1.3% for people aged 60-69 without a learning disability.
Sexual identity
This is an area that is only beginning to be addressed in dementia research, but studies have shown that 41% of older lesbian, gay and bisexual people live alone compared to 28% of heterosexual people; loneliness and social isolation being known risk factors for dementia. Little is known about the risk of dementia among the transgender community, although research undertaken as part of a global study in 2023 suggests that transgender and non-binary adults may be at higher risk of developing Alzheimer’s Disease in later life compared to cisgender men and women. Future research is needed to build the evidence base for specific risk factors that may be contributing to higher overall risk among understudied and underserved gender groups.
Religion or belief
Some culturally specific conceptualisations of dementia view the condition as a normal part of ageing or of having a spiritual, psychological or social cause. This has prevented many groups from identifying dementia as a medical issue and ultimately are not accessing support for dementia.
The role of genetics
NHS England states that, although genes alone are not thought to cause dementia, there are certain genetic factors are involved with some of the less common types. Alzheimer’s Research UK report, ‘Genes and Dementia’, explains that ‘risk genes’ and ‘faulty genes’ could be risk factors in developing dementia. Risk genes are variations in genes that may alter your risk of diseases which may also increase the likelihood of getting dementia. Faulty genes are genes that we inherit from a parent that do not work properly which may affect how your body functions and may cause you to develop certain diseases. Some rare forms of Alzheimer’s and frontotemporal dementia can all be caused by faulty genes, however dementia usually develops because of a combination of genetic and environmental factors such as smoking and a lack of exercise.
What are the risk factors?
Healthy Lifestyles and Behaviours
NHS England consider there is no definite way to prevent all dementia types but there is evidence to show that lifestyle changes can help reduce your risk of developing dementia. Research studies have shown that by acting on the risk factors that people are able to change, a reduction in risk of dementia by up to 30% could be achieved. This could be done by exercising regularly and maintaining a healthy weight, eating a healthy balanced diet, keeping alcohol consumption low, stopping smoking and keeping blood pressure at a healthy level.
Medical conditions and diseases
Healthline describe various factors that can affect your risk of developing dementia, with pre-existing medical conditions and diseases being among them.
According to the Alzheimer’s Society Factsheet, the main health-related risk factors for dementia (especially vascular dementia caused by problems with blood supply to the brain) are:
- type 2 diabetes in mid-life or later,
- high blood pressure in mid-life,
- obesity in mid-life,
- high blood cholesterol levels in mid-life and
- having a cardiovascular disease (which can increase dementia risk by up to two times).
Mild Cognitive Impairment
Mild Cognitive Impairment (MCI) is an intermediate stage between the mental decline expected through normal ageing and more severe mental decline seen in those with dementia; although not all cases of MCI lead to dementia. MCI is not a specific disease but a collective of symptoms such as mild problems with memory and reasoning. As such there is no readily available data at a national or local level, however, Alzheimer’s Society (2014) estimate that MCI affects between 5-20% of those aged 65 and over. Applying this estimate to Wirral’s population indicates that between 3,500 and 14,000 of those aged 65+ in Wirral could have MCI.
Depression
It is possible that depressive symptoms increase dementia risk due to their effect on stress hormones and hippocampal volume. However, it is not clear whether depression is a cause or a symptom of dementia. It was found to be responsible for 4% of the risk of developing dementia.
Hearing loss
According to Alzheimer's Society, people who develop hearing problems during mid-life (aged 40–65) may have an increased risk of developing dementia. Age-related hearing loss is a common condition affecting older people. It often starts with problems hearing what other people say, especially in noisy environments. Symptoms can start gradually and be difficult to notice. This makes early detection and treatment difficult. There is some evidence that, if needed, using hearing aids may reduce cognitive symptoms and slow cognitive decline in people at risk of dementia, though it’s not yet clear if using hearing aids can prevent dementia.
Visual impairment
According to Alzheimer's Research UK, more than one in 10 people over the age of 50 have uncorrected visual impairment. This means problems with sight that haven’t been corrected by wearing glasses, lenses or having surgery or treatment.
In particular, visual impairment caused by cataracts and diabetic retinopathy is associated with an increased risk of dementia. But glaucoma and age-related macular degeneration do not appear to be linked to dementia.
Being long-sighted or short-sighted and not wearing glasses or contact lenses may also increase dementia risk.
A briefing report 'Changes in Perception' January 2021, suggests that eye conditions that can affect visuo-perception include cataracts, glaucoma, macular degeneration and retinal complications from diabetes. Also, certain medications can cause or contribute to problems with vision as well as specific types of dementia can also damage the visual system and cause visuo-perceptual difficulties.
Dementia and inequalities
Life risk factors
In October 2023, the Alzheimer's Research UK published a report ‘Towards Brain Health Equity’ which focused on unequally distributed dementia risk focused on factors out of individual control such as the quality and length of education during childhood, air quality and affordability of a healthy lifestyle. Exposure to risk factors is not equally distributed among society, and unfairly burdens the UK’s most deprived communities and regions with poor brain health, increased dementia risk and reduced life expectancy.
Social isolation
Social isolation is thought to increase a person’s risk of dementia by about 60%, however is can also be a consequence of dementia.
Social isolation can relate to someone’s marital status as married people often have more social contact with others than single people. Studies show that lifelong single people are more likely to develop dementia than those who are married. Widowed people are also slightly more likely to develop dementia.
Social contact is significantly increased in married people, and there are other factors that may reduce the dementia risk for married people. Married people are more likely to be healthier and have more education.
Even when accounting for these factors, social isolation is shown to increase dementia risk. There is also known to be a strong connection between high social contact later in life and memory and thinking skills.
It is not known why social isolation increases dementia risk, but it could be due to it’s link to a host of other health and social factors. Lonely people are more likely to drink heavily, smoke, not exercise and be overweight and have heart problems all of which increase dementia risk.
Socio-economic gradients in risks
There are several dementia risk factors related to socio-economic position such as a lack of physical activity and early education. There is also a strong link between cigarette smoking and socio-economic group. Smoking has been identified as the single biggest cause of inequality in death rates between affluent and poor population groups in the UK. Some studies suggest that it can double the risk of developing dementia.
Low levels of education
Less time in education - specifically, no secondary school education – was considered responsible for 7.5% of the risk of developing dementia. However, and for social isolation, it is important to note that to add up the percentage risk of all these factors, they only account for about 35% of the overall risk of getting dementia. This means about 65% of the risk is still due to factors out of an individual’s control, such as ageing and family history.
Societal barriers
Some individuals and populations face significant societal barriers to engaging in dementia risk-reduction behaviours. With the evolution of the dementia prevention field, there is an argument to broaden the approach from identifying individual risk factors towards addressing inclusive and globally effective intervention strategies.
[AD1]Local data to confirm this?
Impact of dementia on individuals, carers and families
Living with dementia
Dementia has a significant impact on an individual’s health and quality of life. It can result in a range of health and social problems which can be challenging for the person with dementia, their carers, and health and social care professionals. The prognosis for a person with dementia varies depending on the cause of the dementia and the pattern of symptoms.
As the dementia progresses, people with dementia can experience severe cognitive impairment and memory loss. Psychological and behavioural problems such as depression, disorientation, and aggression may also develop and get worse over time which can be difficult to manage. These ‘distressed’ behaviours may be exhibited due to pain, anxiety, fear or may be a reaction to external factors such as staff behaviour or poor physical environments. Establishing what is causing the distress and dealing with these issues usually results in being able to better manage distressed behaviours.
The Alzheimer’s Society’s 2025 report ‘Lived Experiences of Dementia’ states that large proportions of people with dementia feel unsupported and do not feel part of their local community.
The findings of this report also expose gaps in care, diagnosis and public awareness;
- 73% of people with dementia feel anxious or worried to be living with symptoms of dementia while 42% felt ashamed or stigmatised to be living with them.
- Less than 2 in 5 survey respondents think healthcare or social care support for people living with dementia is important to the government.
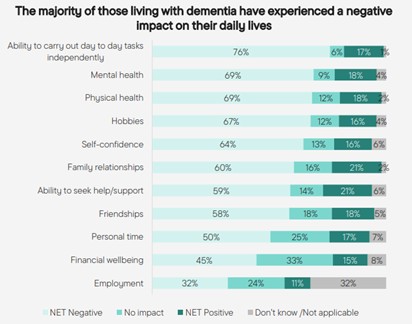
- 69% of people with dementia reported a negative impact on their physical health and their mental health.
In addition to this, as life expectancy increases for people with complex disabilities, carers for these individuals will be caring for longer and may develop dementia themselves; affecting their ability to provide care. Many parent carers are single parents, which is an additional risk factor delaying identification.
Whilst experiences of treatment and interventions is largely positive, access can be difficult. The majority of people who have been offered any drug and/ or non-drug treatments have found them beneficial. Despite this, access to these types of treatments is varied, with over a third of those with dementia not having been offered a non-drug treatment, and one in five not having been offered a drug treatment.
Impact on carers
According to Dementia Carers Count, in 2024 there were over 5 million unpaid carers in England and Wales. Nearly one in five was caring for someone living with dementia – most often a spouse or partner or a parent. The 2025 Dementia Carers Count Survey found that 54% of respondents were caring 24/7, with 18% caring 15 hours a week, 13% up to 30 hours a week, and 8% up to 45 hours a week.
The Alzheimer’s Society’s 2025 report ‘Lived Experiences of Dementia’ states that seven in ten (70%) who care for someone living with dementia have experienced a negative impact on their daily lives as a result of caring for someone. Just under half (46%) say that they spend less time doing the activities that they enjoy. Many unpaid carers have also experienced a negative impact on their mental health (37%) or physical health (24%).
For some though, caring for the person living with dementia has been a positive experience as they feel closer to the person who they are caring for (39%) or they feel a sense of fulfilment (33%).
Research has found that those providing care are more likely to be in poor health than those not providing care. Caregivers often experience high levels of stress, anxiety and depression as well as facing the physical toll of neglecting their own wellbeing while focusing on the needs of the person with dementia.
In addition to poorer physical and mental health, carers can often suffer from social deprivation, isolation, fewer opportunities for paid employment or education, or having time to themselves or with friends. For young carers, it can often mean life chances are severely limited.
Caring responsibilities are likely to have a significant impact on carers’ quality of life which can be compounded for those looking after somebody with dementia than carers generally.
The Dementia Carers Count survey highlights how over three-quarters of dementia carers, who are looking after a spouse, partner or parent, have no alternative care plan in place for when they can’t care for them – for example, should they need to access care and treatment themselves. The survey also reported that 85% of unpaid carers of people with dementia have reached crisis point, with 52% stating they receive no support at all.
Stigma and Discrimination
Stigma is a negative or unfair belief based on a stereotype about a person – such as their age, race, religion, gender, sexual orientation or disability. Sometimes, people with dementia feel stigma towards themselves – for example, they might think they are ‘stupid’ or ‘a burden’ due to their diagnosis. This is called self-stigma. When someone lives with dementia, they may experience stigma or discrimination. This is usually because of people’s negative perceptions of what dementia is, who it affects, and how it affects them. This may lead to the person being treated differently, or sometimes, people taking advantage of them. (Dementia UK, March 2026)
Both stigma from other people and self-stigma can be hard to deal with and can have a negative impact on a person living with dementia. Stigma and a lack of knowledge about dementia are barriers to timely diagnosis of the condition and to appropriate treatment and care.
The Dementia Services Development Centre at the University of Stirling states that breaking the stigma of dementia requires collective effort—through education, empathy, and policy changes. Strategies such as education and awareness campaigns, encouraging open conversations, promoting inclusivity and supporting care partners can work to reduce stigma against those living with dementia.
Discrimination is poor or unfair treatment that often results from stigma and negative stereotypes. People may face discrimination for a variety of reasons, including race, gender, age, sexuality and disability.
People with dementia often face discrimination based on stigma and biased opinions, for example, beliefs that people with dementia should not be left alone, cannot be trusted to make decisions, or cannot look after themselves.
What steps can be taken to reduce the risk of developing dementia?
NHS England suggests that there's no certain way to prevent all types of dementia, as researchers are still investigating how the condition develops. However, there's good evidence that a healthy lifestyle can help reduce risk of developing dementia with age.
This means the risk of dementia can be reduced by:
- eating a balanced diet
- maintaining a healthy weight
- exercising regularly
- keeping alcohol within recommended limits
- stopping smoking
- keeping your blood pressure at a healthy level
Protecting eyesight and hearing, by correcting vision loss and using hearing aids, has also been shown to reduce the risk of dementia to the level of a person with normal hearing or sight.
Traumatic head injuries can also start a process in the brain where the substances that cause Alzheimer’s disease build up around the injured area. Wearing protective headgear in situations where there is a higher-than-normal risk of head injury – for example, riding a bike, working on a building site, horse-riding or playing cricket – can help to reduce this risk.
Cognitive concerns in those who have played contact sports (such as rugby) for a long period of time has been subject to research in recent years. Further information of these findings can be found in this article published by Imperial College London.
The NHS Health Check programme helps in finding early signs to identify who is at higher risk of certain health problems that can increase dementia risk and help them to prevent and manage these health conditions. These include:
- coronary heart disease
- diabetes
- kidney disease
- stroke
What support services are available?
The Dementia 100 self assessment will provide a wider understanding of the current services that are meeting the needs of people living with dementia and their carers.
This information will be shared here on the this page as it becomes available.
Additional content
Relevant and related National and local strategies
-
Cheshire and Merseyside ICB Dementia Strategy to be added
-
C&M Population Health Improvement Plan Dementia Priorities to be added
-
LCR Dementia Friendly Pledges to be added
-
NHS 10 Year Plan 10 Year Health Plan for England: fit for the future - GOV.UK
-
NHS England Well Pathway NHS England » Dementia wellbeing pathway
-
Major Conditions Strategy Major conditions strategy: case for change and our strategic framework - GOV.UK
-
Wirral Place Dementia Strategy 2022-25 (out of date but maybe a useful reference doc) wirral-dementia-strategy-2022-2025-march-22-final.pdf
Previous Content
Past Needs Assessments
Further information
From previous JSNA iterations
Dementia Profile for Wirral
This can be found on the Public Health England website.
Dementia: assessment, management and support for people living with dementia and their carers
Guidance and guidelines from NICE (June 2018)
This NICE guideline covers diagnosing and managing dementia (including Alzheimer’s disease). It aims to improve care by making recommendations on training staff and helping carers to support people living with dementia.
MODEM Dementia Evidence Database
The Dementia Evidence Toolkit is for commissioners, care providers, people working in health and social care and people with dementia and their families. The toolkit will help those planning and shaping services and treatments for people with dementia and their carers make informed decisions about which services and treatments to provide and how much they cost.
Dementia and Mental Health Resources
NHS England have provided Mental Health Resources in the form of information, tools and guidance to support mental health commissioning and the transformation of services in relation to dementia. Access the NHS England website for more information.
Dementia does not discriminate - The experience of Black, Asian and minority ethnic communities (2013)
The All-Party Parliamentary Group on Dementia investigated the experiences of people from BAME communities with dementia. As this report sets out, the number of individuals with dementia from these communities will increase rapidly in the coming decades. Our inquiry heard about high-quality services that were tailored to support people with dementia from BAME communities. But we uncovered that these services are too few and far between, and many people struggle on with too little support from the NHS or local government.
Listening to people with dementia and their carers (2016)
This new listening programme was introduced to find out more about the experiences of people with dementia and their carers starts in England
Dementia support programme, the Joseph Rowntree Foundation (JRF) (November 2015)
Dementia Friendly Communities: sharing learning from Bradford and York here
As part of this programme JRF has published How can we make our cities dementia friendly: sharing the learning from Bradford and York. These reports identify key messages from two independent evaluations of areas that are relatively advanced in their dementia friendly community (DFC) developments.
How can and should UK society adjust to dementia? (July 2015)
This Joseph Rowntree Foundation paper explores the application of the ‘social model’ of disability to dementia. It aims to stimulate debate about new ways forward in understanding, and ways to meet the needs of the growing number of people living with dementia.
Background information related to Dementia
This can be found on the Public Health England website.
Government Policy on Dementia
This can be found on the GOV.uk website and the Dementia Challenge can be found on The National Archives website.
Dementia maps of variation and state of the nation report
Department of Health has published maps of variation and state of the nation report into the range and provision of dementia care and support services in England.
The Carers Call to Action
Dementia Action Alliance have produced a PDF version of their booklet written by carers for carers of people living with dementia about their shared vision called The Carers' Call to Action. They have also produced a 20 point checklist to identify where the gaps and the strengths are in local areas.
Improving care for people with dementia
Government website carrying a range of information to help support the care of people with dementia. Access the GOV.uk website for more information.